On July 9-10, The American Health Quality Association (AHQA) convened national partners working to improve healthcare quality in Baltimore, MD for the 2018 AHQA Quality Summit. Honored to have attended as a James Q. Cannon Fellow, I spent these two days learning from expert speakers and peers about strategies for continued healthcare quality improvement through community awareness, innovation and collaboration.
Being a first-time guest to Baltimore I wandered nearby Inner Harbor with our group on Sunday evening and—in true tourist fashion—gaped at the Maryland Science Center, the World Trade Center Institute Baltimore, the USS Constellation, Camden Yards and much more. I also tried the much-acclaimed crab cakes which, for the record, absolutely live up to the hype.
Over the next two days I made countless connections between my work as part of Lake Superior Quality Innovation Network (QIN)(link is external) in Michigan and the impactful work being done by fellow attendees and presenters nationwide. Below are takeaways from sessions I attended including new perspectives to apply to my work as a member of Lake Superior QIN. As these summaries are somewhat brief, I encourage you to visit the 2018 AHQA Quality Summit webpage for a complete list of sessions and presentation slides.
The Science of Burnout and Well-being in Healthcare: How Other People Matter, Kathryn C. Adair, Ph.D.
Dr. Adair, social psychologist with the Duke Patient Safety Center(link is external), began the Summit by discussing the science of burnout and wellbeing in healthcare. With many demands and limited time facing healthcare providers in our current system, this topic was extremely timely and inspired conversation throughout the rest of the Summit. Study data presented during this session drove home the quiet ubiquity of healthcare provider burnout, specifically in:
- Critical care nurses: half are emotionally exhausted, two out of three have difficulty sleeping, and one out of four are clinically depressed.
- Surgeons: 8.9 percent reported making a major medical error in the previous three months (reporting an error had significant correlations with all three domains of burnout).
- Medical students: half are burned out, nearly half report excessive fatigue and 10% percent have suicidal ideation (compared to 3.7 percent in the general population).
In addition to the impact of burnout Dr. Adair also discussed environmental correlates that act as buffers, or “burnout band aids,” including (but not limited to) social support, a positive learning environment, satisfaction in conversation with others and positive working relationships. To address and prevent healthcare provider burnout—as well as strengthen workforce resilience—Dr. Adair recommended implementing both institutional and personal interventions.
Personal reflections:
- “Focus determines your reality” and “perceptions are influenced by how you feel” – our internal environments influence what we contribute to and take from daily interactions.
- As Quality Innovation Network-Quality Improvement Organization (QIN-QIO) staff, we are in a prime position to reduce healthcare provider burnout by aligning initiatives with clients’ priorities including quality reporting programs, unique community needs and payment mechanisms.
Takeaways for my work as part of Lake Superior QIN:
- Support provider and partner resilience to prevent burnout and promote project sustainability
- Continue to provide technical assistance (TA) that accounts for and optimizes workflow.
- Recognize success in fostering teamwork and positive working environments.
- Encourage “positive rounding” in internal and client meetings/huddles to recognize what’s going well and individual/organizational successes.
Find strategies, slides and references from this presentation here.
Driving Change and Moving Toward the Future: Looking Ahead for the QIO Program, Jeneen Iwugo, MPA and Paul McGann, M.D.
Jeneen Iwugo, MPA and Paul McGann, M.D. from the Quality Improvement & Innovation Group in the Center for Clinical Standards and Quality at CMS discussed results achieved from the current 11thScope of Work to date and future directions for the QIO program(link is external).
National progress made so far in the 11th Scope of Work includes:
- 350,000 fewer patient harms, 8,000 lives saved and more than 2.9 billion in cost savings.
- 18.7 percent reduction in antipsychotic medication use in residents living in long-term care facilities.
- 91 percent of MIPS eligible clinicians, 98 percent of accountable care organizations and 94 percent of MIPS eligible clinicians in rural practices submitted data for the 2017 performance year.
- Prevented 46,000 hospital readmissions and contributed to $600 in cost savings throughout 387 communities.
- Educated 5,300 providers and 48,662 Medicare beneficiaries completing diabetes self-management education.
With more to come!
Potential focus areas for the next Scope of Work were shared including workforce burden reduction, improving behavioral health including opioid abuse, improving chronic disease management (cardiovascular, diabetes, CKD-ESRD), increasing patient safety, increasing quality of care transitions and long-term care. Proposed focus areas resulted from public input and CMS’ Agency priorities and would incorporate rural health, vulnerable populations and patient and family engagement as cross-cutting priorities.
Find more QIN-QIO programming results, future directions and slides from this presentation here.
Reducing Provider Burden with an Integrated Outpatient Services Approach, Sharon Donnelly, M.S. and Sharon Phelps, R.N., BSN, CPHIMS
Sharon Phelps from Mountain-Pacific Quality Health Foundation(link is external) and Sharon Donnelly from Qualis Health(link is external)/HealthInsight(link is external) described their many partnerships, collaborations and considerations in working with providers on their QIN-QIO task work. A two-pronged approach presented consistent focus on reducing burden for providers and internal staff, including:
|
Reducing Provider Burden |
Reducing Internal Burden |
|
|
|
|
|
|
|
|
Programming for outpatient providers is streamlined by grouping interventions into four core categories—advance care planning, annual wellness visit, transitional care management and chronic care management—within a framework of current and new payment mechanisms. The session described work designs that incorporate collaboration, alignment, big picture thinking and technology solutions that successfully break down programming silos and build on clients’ priorities and goals.
Takeaways for my work as part of Lake Superior QIN:
- Continue to regionalize task TA to promote consistency and meaningful evaluation.
- Support burden reduction by optimizing health information technology in practices and empowering providers to use available EHR functionalities to input and act on data.
Find more on this integrated services approach and slides from this presentation here.
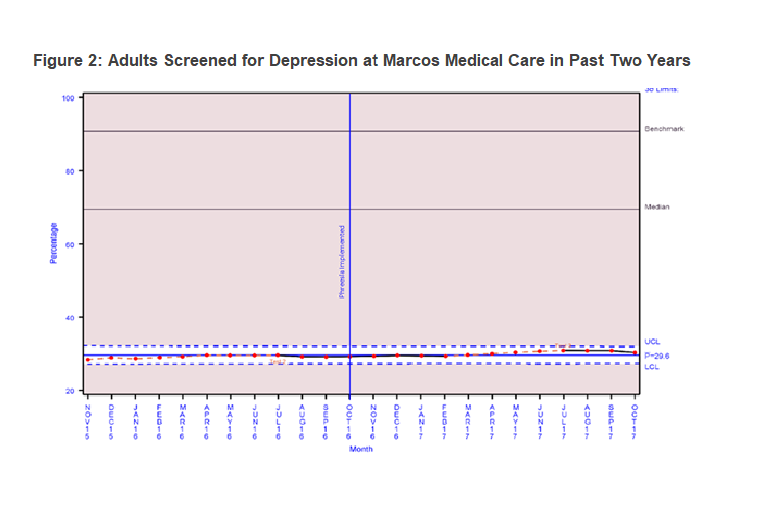
A QIN-QIO Collaborates with Academia: Engaging Small Practices in Blood Pressure Control, Joanne Vanterpool, MBA and Susan Hollander, MPH, CPHQ
During this session, Susan and Joanne presented their work on Project Implementing Million Hearts for Provider and Community Transformation (IMPACT).(link is external) Started in 2014, this initiative centers on Million Hearts®(link is external) goals with a focus on improving blood pressure control and cardiovascular outcomes in the South Asian community cared for in primary care settings across New York City. Project partners provide TA and subject matter expertise to targeted practices, including:
- Evaluating use of community health workers (CHWs) and EHR functionalities and interventions.
- Testing and implementing CHW and EHR-based tools targeting Million Hearts® goals.
- Developing and implementing culturally tailored provider training programs to empower direct care staff to improve hypertension control.
Personal reflections:
- A theme continues – Joanne and Susan described an approach to programming that aligns initiatives and incentive programs and supports optimizing practices’ resources (improving patient care and outcomes + minimizing burden).
Takeaways for my work as part of Lake Superior QIN:
- Utilize lean approaches to drill down to root causes of providers’ challenges in caring for patients with chronic conditions.
- Example: is a practice’s percentage of patients with controlled blood pressure (BP) (NQF 0018) persistently low?
- Asking The Five Whys(link is external) may reveal that inconsistent staff technique for manual BP measurement may be overestimating patients’ BP and assistance is needed to facilitate competency training.
- Example based on findings from a root cause analysis in Michigan (before my time) that contributed to regional collaboration on Lake Superior QIN’s Hypertension Management Toolkit(link is external).
- Example: is a practice’s percentage of patients with controlled blood pressure (BP) (NQF 0018) persistently low?
Find more on programming approach and Project IMPACT here.
Overarching theme – the opioid epidemic
In addition to burden reduction, the opioid epidemic(link is external) was also a common theme throughout multiple sessions, including:
- Opioid Performance Improvement Project in Nursing Homes: Utilizing a Virtual Collaborative to Drive Results, with Amanda Ryan, PharmD, BCGP.
- Reduction in Opioid Prescribing Through Evidence-Based Prescribing Guidelines, with Joceline Vu, M.D. and Gloria Pizzo, R.N., BSN.
- Opioid Guardianship: Combating the Opioid Crisis, with Sarah Derr, PharmD and Meg Nugent, MHA, R.N.
- CMS’ Jeneen Iwugo, MPA and Paul McGann, M.D. also shared strategies(link is external) employed within a current Special Innovation Project to address opioid misuse and behavioral health disorders in Southwestern Ohio.
These sessions issued a clear call to action to attendees to continue national work with healthcare providers on prevention efforts and rapid response projects to support quality care and patient safety.
Connecting and collaborating
In addition to presentations highlighting quality improvement program successes, I attended a brainstorming breakout session called “Collaborate & Solve!”, facilitated by AHQA Executive Director, Alison Teitelbaum, M.S., MPH, CAE. During this session, we identified common challenges in our work and split up into small groups to discuss lessons learned. My group explored work silos both within our organizations and with stakeholders:
- The issue: groups don’t always see value in collaboration (possibly due to organization cultures, fear of change, etc.).
- Brainstorming – what we have seen work for silo breakdown:
- Researching the landscape and taking advantage of existing groups, advisory boards and coalitions (statewide and regional).
- Listening to partner and stakeholder experiences (learn vs. reinventing the wheel).
- Coordinating so that joint efforts become comfortable and keeping communication open (regular touch base calls) about what is going on and continued interest in partnership.
- Uniting under the understanding that we can’t reach everyone we want to reach without partnering.
One point presented by one of my fellow brainstormers stuck with me both personally and for my work as part of Lake Superior QIN: “It’s amazing what you can accomplish when you don’t care who gets the credit” – Harry Truman.
Find additional small group topics and discussion notes here.
Reflections and thanks
As I reflect on my first experience attending the AHQA Quality Summit, I’m left with broadened perspectives and a great sense of purpose and gratitude. I want to express sincere thanks first to the AHQA Board of Directors and all involved in the development of the James Q. Cannon Memorial Scholarship for the opportunity to attend this year’s event and for investing in early career professionals. Thank you to all those involved in the planning and successful execution of the 2018 Quality Summit as well as the speakers who dedicated their time and expertise to make this a truly educational and engaging event. Finally, thank you to my fellow attendees for inspiring me to a wider perspective on our work and its continued importance – I hope we meet again at future summits and out in the field with our boots on the ground, continuing to support quality healthcare nationwide.

 The conference opened up with K. Carrie Adair, from Duke University who presented on
The conference opened up with K. Carrie Adair, from Duke University who presented on  Sara Derr, PharmD and Meg Nugent, MHA, RN presented on behalf of the Iowa Healthcare Collaborative on the IHC Opioid Guardianship Project. Another stand out for me in opioids, was Amanda Ryan, PharmD, BCGP from Atom Alliance’s presentation on
Sara Derr, PharmD and Meg Nugent, MHA, RN presented on behalf of the Iowa Healthcare Collaborative on the IHC Opioid Guardianship Project. Another stand out for me in opioids, was Amanda Ryan, PharmD, BCGP from Atom Alliance’s presentation on Improving the quality of healthcare is meaningful, important, life-changing work, but it can also be very challenging. As quality improvement professionals, supporting one another through peer-to-peer sharing and collaborative relationships is critical to success. It takes all of us with unique perspectives and expertise to facilitate the changes needed to continue making healthcare better.
Improving the quality of healthcare is meaningful, important, life-changing work, but it can also be very challenging. As quality improvement professionals, supporting one another through peer-to-peer sharing and collaborative relationships is critical to success. It takes all of us with unique perspectives and expertise to facilitate the changes needed to continue making healthcare better.